COVID-19 | Corona Virus: Epidemiology, Pathophysiology, Diagnostics
Mar 23, 2020Very good engineers, in this video we are going to talk about
covid
19 or the newcorona
virus
that was discovered in 2019. I want you to know that in this video that we are doing today all the information that we are going to talk about. About is updated on March 15, 2020. So I just want you to know that also this video is for educational purposes only. We will have a medical disclaimer pop-up here. Let's go ahead and get off to a good start. guys so let's go ahead and start with this conference oncovid
19 so again I want you to remember that we are going to do this video here on March 15, 2020 obviously things could change from now on to the future as those things change, we will try to Continue to keep you updated with future videos to go into more detail about these things, okay, but again, this is okay as of now, so what should we know about thecorona
virus
?
Well, we know that the coronavirus is this coronavirus 2019. Well, it is similar specifically to the sars virus, if you remember what it was, there was an outbreak called severe acute respiratory distress syndrome and it was coronavirus specifically in 2002 and what happened is they believed that this virus actually had the ability to jump from a bat, well, from that bat it mutated in such a way that it can then infect another host, another intermediate host, so it started with a bat from the bat and then maybe it transferred to what we think is a civet and then from that civilization it mutated enough to be able to infect a human because coronaviruses are naturally quite benign and don't cause many significant effects on humans, maybe you just know your viral rhinitis , viral pharyngitis, viral laryngitis. but rarely are they going to cause this type of severe acute respiratory distress syndrome, but again, if they mutate enough when they pass through some type of animal reservoir, they can mutate enough to be able to cause serious infection in humans and that's what The sars virus made copper in 2002 a couple of years later actually a decade later in 2012 it happened again where the coronavirus had the ability to mutate again where we have a bat where we believe that is again the animal reservoir where the virus mutated and then it was transmitted to what we think is a camel, so from bat to camel as the next intermediate host and then from there it mutated enough to be able to infect a human.

More Interesting Facts About,
covid 19 corona virus epidemiology pathophysiology diagnostics...
Well, this is the mers virus and again this is the Middle East respiratory distress syndrome which occurred in 2012. Let's now go to 2019 where we now talk about the coronavirus, particularly covid19, which was the coronavirus discovered in 2019. Again we believe that this actual virus underwent a mutation through this zoonosis, so we have a bat that mutated within the bat and then actually had. We're still not completely sure about the ability to mutate within another animal as an intermediate host, but we think it could be what's called a pangolin, so they think this virus jumped to a bat when its reservoir mutated enough and it was transferred. to a pangolin.

It has mutated enough that it can now infect a human and cause covid19. Well, what is the new coronavirus discovered in 2019? Here's what we know about this virus now. Another thing we have to understand about this virus is not only its zoanosis effect, but we should also know some of the case fatality rates because this is becoming a big concern in society right now. Everyone is very afraid of the coronavirus and again, we don't want to overreact, but we want to make sure we don't underreact. to this virus because it is a very serious virus to give you a little example of the fatality rates if we take the sars virus in 2002 the fatality rate is again the total number of cases at the bottom so if the guys want to remember the formula, a very simple formula: the number of deaths divided by the total number of cases, okay, and then multiply it by a hundred so you can see that this virus, the sars virus, in 2002 had 8,000 cases in total with 800 deaths , which gives us a case fatality rate of 10 which is pretty decent, move on to the next one, the mers virus in 2012. 850 died where there were 2,500 cases in total, which will give us a case fatality rate of 34 percent, move here to covid19 as of March 15, 2020. we have 153,517 cases, okay, this is worldwide with 5,735 deaths, which gives us 3.7 percent now, many resources, global health organizations, the cdc, different things like that say that this number could technically be even lower, you have to remember that there are many people who are asymptomatic with this virus are fine, in other words, they do not present the classic symptoms that we would see with the coronavirus, so if They are asymptomatic, technically they would be one of the cases, but it is possible that they do not present them.

They might not go to the hospital to get tested and test positive for coronavirus, so technically, if you think about it, there could be thousands and thousands more cases where people are simply asymptomatic and think they have a common cold. or maybe flu, but they actually have the coronavirus and think about it since this denominator increases the more cases we have, that case fatality rate could technically go down and that's what you want to think about right now, yeah, it's scary how much cases that we have and the deaths, but again, this denominator, technically it could be a little bit larger, okay, that's what I want you to understand right now about the basics of the coronavirus when it comes to the zoonotic effects, in other words , how this coronavirus mutated enough to be able to infect humans. and causes severe acute respiratory distress syndrome.
Okay, if you understand this through the stars, it's pretty much the same thing: the bat was pretty much the primary reservoir animal that then passed it on to an intermediate host, which we believe at this point. be a pangolin now, how come these important pangolins? According to many researches it was shown that actually its scales have healing properties, which is why it is highly trafficked around the world, that is what also makes it very dangerous and therefore increases the risk of a pandemic. that again we need to be careful when it comes to this and just realize that this intermediate host could be one of the things that actually allows this mutation of the virus and allows it to affect humans in such a way.
Alright, let's move on to the next epidemiological fact, when we talk about the coronavirus, when we talk about the coronavirus, we have to talk about what is called r zero, the r zero means reproductive ratio, okay, a special way of saying that this is the degree of the ability to spread, that's really it, it's how much can one person infect, how many people can one person infect, that's a simple way of saying it, so if I take, for example, let's say here's this person, okay, patient number one, has the covid19 coronavirus. infected, you're around other people, you're in the same room with a group of people, okay, if you sneeze or cough and spread those respiratory droplets that could be in the air and somehow get on the mucous membranes of people nearby, how many could potentially? infect they say it can infect three people, therefore, the arnott of covid19 is said to be two to three, it could even be higher.
We'll talk about that in a moment what I mean by that so again what's the r nothing for covid19 we think it's between two and three let's take the worst case scenario and say it's three okay one person can infect three people, so it starts with one person infecting three people, these three people, each one infects three more people, that gives us nine patients now infected with coverage 19. now these nine people can go and infect three people each, how many are those 27? So you can see how this is an exponential increase if we look at this on a graph when you look at nothing from covid 19 let's do it here in blue if you look here they're not on the axis and what are you going to see you're going to see this number is going to increase true it's going to be exponential this is an exponential growth if we compare the r nothing of influenza which is around 1.3 approximately, let's round it up to one and say that a person has the ability to infect another person, so if this person is infected with influenza, they will be will transmit it to another person, one person will transmit it to the next, who will transmit it to the next person, so you can know right now just by comparing influenza and kovid 19 that this has a much greater ability to spread, whereas this has a much smaller spread. capacity okay, so if we were to compare, this is exponential, this is decreasing or this is pretty much the same, it's a flat line, it's a flat line, so we should see that the r zero here is straight, what would we prefer?
This should look like less than one, preferably we don't want this to have such a high extension, so if we had a perfect scenario, we would love for this to start decreasing, how do we do it? How do we get the r to nothing? fall? We will be quarantining, staying away from large crowds, trying to decrease that ability to spread by spreading respiratory droplets, making sure we wash our hands, making sure we don't touch our T-zone and by doing that, and quarantining. yourself and staying away from large crowds, we can potentially decrease that ability to spread, that's what we want with this virus, so currently you can see how nothing is greater than one that allows for this exponential growth, that's why there are so many cases compared to something. like the flu, which one is one and what we would like what we would prefer is nothing less than one.
Well, the last thing I have to talk about here because it not only determines the rate of transmission or the degree of spread, but there is also another factor. and this is called series interval, so if it is known as series interval, a special and very simple way of describing this and let's say here is patient one, well, patient one develops symptoms well and let's say that from the day zero you developed symptoms all the way up to day 14. Okay, let's say you have symptoms for 14 days, so this is when the symptoms stop, this is when the symptoms start, let's say at some point during your infection period you transmit that virus to someone else, so let's call this x2, right? here is x1 patient one, patient two, this person gets infected, let's say somewhere right here, maybe it's day two, okay, maybe day two, somehow at that moment, this pa patient x patient one comes into contact with patient two and from that point their symptoms start, so now while it's day zero and let's say they go through a fourteen day period of this actual infection from this point to this point from the onset symptoms from patient one to patient two's onset symptoms, that's our series interval now the shorter it is, the more dangerous the virus, the bigger the better, the less risk of becoming such a high transmission rate, so , what is the series interval for covid19?
It really depends, it depends on the source you're looking at. let's say it's between five and some will say between 7.5 if you take influenza for example, it's actually about 2.5 around that, so what does that mean? It means that the time of symptom onset in patient one is right from when that person is actually infected to patient two's symptoms start to develop in a period of 7.5 days, while the infection period of patient 1, who is infected with influenza from the onset of symptoms to the onset of symptoms of patient 2, is about 2.5 days, why would it be dangerous if you have a high r knot in a really low series interval within a small amount of time, so imagine here one person infects three, it took 7.5 days from 3 to 9, 7.5 days from 9 to 27, that's 7.5 days spread over a longer period .
Fortunately, however, if we imagine 2.5 days of symptom onset from patient one to patient two, this would be extremely high. Well, there would be a very high spread of transmission at a very fast rate, for which we should at least be grateful. for now the si is relatively high and our zero r is also high, this is the unfortunate aspect, but be thankful at least that we have a high series interval with the zero r here, this one is relatively low, but it has a relatively high series interval low. then it can spread quite quickly, but in this case there is more capacity for spread and a greater number of infectious cases, so they think that there are two forms of correct fecal oral route potentially and that respiratory droplets, such as fecal or rods, are one of the ways that we think that Actually, this could be transmitted well, and what happens with this is that if someone goes to the bathroom, they eliminate the virus, you know, they wipe their butt, they don't wash their hands completely and goes and touches other surfaces inside the bathroom, someone else comes. they touch those surfaces and potentially, you know,they get inoculated with the virus, that's one way we think it could happen.
Well, other things that we also have to remember is that, if there are certain things, if someone lives in an apartment. building where there is a faulty plumbing system where certain plumbing is correct, so perhaps fecal material from someone who is actually an infected individual has the ability to spread through a faulty pipe or drainage system to another room of the apartment and allowing those viruses to also infect certain areas and surfaces within another bathroom, that is another way, so again the oral fecal rod is one way of transmitting the virus and the other is coughing and sneezing so that it can be via air or through respiratory droplets.
Now one of the things that they say about these respiratory droplets is that they have the potential to spread and actually infect a person, maybe within three to six feet, well, another thing is that they think that these respiratory droplets could linger in the surfaces and actually survive for about 24 hours and if someone goes and touches that surface and then touches one of their mucous membranes, they have the ability to inoculate themselves again. The most recent research is also newer. They also say it could potentially be in the air for potentially three hours, so if someone actually coughs or sneezes and then someone walks through that area potentially within a three hour period, they could also become inoculated with the virus, so again, the oral fecal route and respiratory droplets are how we think this is potentially spreading, another really interesting thing is that they can also be asymptomatic carriers, so sometimes if someone isn't actually showing symptoms, they potentially have the ability to spread this real virus, so that's what's also very stressful.
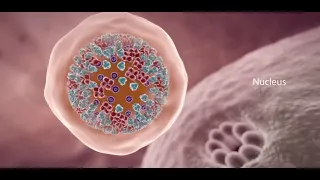
Okay, now what happens is the virus enters the respiratory system just once it enters the respiratory system, it loves to attack the alveoli, so what we're going to do is we're going to get close to this portion of the lungs and take a good look at the alveoli. , so once the virus gets to this area, what does it do well? The first thing it's going to do is come here and attach itself to these type 2 pneumocytes that you know, inside the actual alveolus, you have two. different types of cells, type 1 pneumocytes that will be for gas exchange and type 2 pneumocytes, which will be your structures that will produce surfactant and that's important to remember because what the surfactant does decreases the surface tension within these alveoli and reduces that. collapse pressure that will come into play in a second, so what we're going to do is watch as this virus infects this cell and uses the cellular machinery to produce more viral particles and then wreak havoc on the respiratory system. system, so if we take a look here, we have our virus right now, this virus has different types of spike proteins, one of the specific spike proteins that we have seen that is actually a little bit significant here is this rose and Call this the s-peak, okay, we call it s-bike, why is it so important?
Well, these spikes in this covid19 virus, okay, the new coronavirus discovered in 2019 binds to specific receptors on type 2 pneumocytes, what is this actual receptor? this receptor is called angiotensin converting enzyme type 2. it binds to this and when it binds to this it allows the virus to be absorbed and absorbed by the cell, once it enters the cell it releases its RNA because here we have a virus of positive sense single-stranded RNA, it releases the single-stranded RNA into the actual cytoplasm of this type 2 pneumocyte once it is released, guess what it does, it can do a couple of things, one is that it can actually use the ribosomes of the host cells and if it uses the host cell's ribosomes, then it can be what takes the mRNA and turns it into proteins.
What is translation called? So what can happen is we can go through what's called translation and we're going to convert this single-stranded RNA. write this, what do we have here? single-stranded RNA. We're going to turn this translated into specific protein molecules, so we're just going to draw a bunch of different proteins. Here different polyproteins. Here is a polyprotein. Here is a polyprotein. Heck, let's draw another polyprotein. and it's going to be doing a lot of different things right now from here after it synthesizes these proteins, guess what else it can do? Actually, it's actually really very interesting, you see that ssrna, the positive sense, positive sense, single-stranded RNA, has the potential to use another enzyme called RNA-dependent RNA polymerase, so what is this enzyme called here?
It is called RNA-dependent RNA polymerase. What does that mean? Takes RNA and synthesizes RNA. So what are we going to do here? Oh, this is great, guys, look, this is needed. single-stranded RNA and turns it into more RNA, so now from this I have a single-stranded RNA. I'm going to make more copies of this single-stranded RNA. Well, in a positive sense, now here are my polyproteins. I need to make these polyproteins become all the components of my virus that make up my nucleocapsid, specific enzymes, my spike proteins, so I need specific enzymes that will proteolyze these polyproteins at the different individual points that I need to create this whole viral structure, so we have other enzymes here, okay, we have enzymes.
Let's choose a blue color, this enzyme will be ace proteins and there is a specific type of ace proteins that will proteolytically cleave these polyproteins into the different viral components that make up the nucleocapsid enzymes and the spike proteins. Now look what I used. the cell's RNA-dependent RNA polymerase and use the cell's ribosome to produce proteins that will form the components of the viral protein structure at that time, I synthesized a ton of RNA, what happens if I combine these two? I combined all of these real nucleocapsids. The spike proteins, the enzymes with the single-stranded RNA take it in and then I get rid of this type 2 pneumocyte.
I just produced tons of virus particles and in the process I'm destroying this type 2 pneumocyte if I cause damage to it. What is that going to do? There are a couple of things that are going to happen. One of the things here is that this type 2 pneumocyte will start to become damaged, so it will release specific inflammatory mediators. Guess what those inflammatory mediators are going to do? We are going to tell the macrophage. The macrophage, once stimulated, starts secreting specific cytokines that cause a lot of problems. One is called interleukin, a large one is called interleukin-6, and another is called tumor necrotic factor alpha.
What the guys do is they actually come here into the bloodstream and cause these endothelial cells to dilate, so it will cause the smooth muscle to actually cause the smooth muscle to dilate, but it increases capillary permeability by causing contraction. of the endothelial cells and then by doing that you increase the permeability so now look, I'm going to release all these different inflammatory mediators, what's going to happen in response to that? I'm going to cause vasodilation and I'm going to cause an increase in capillary permeability if you do that, what's going to happen now? All of this fluid, all of my plasma, will begin to flow and leak into the interstitial spaces and potentially into the alveoli.
As all this fluid starts to build up outside the alveoli, this will lead me to try to compress the alveoli. On top of that, some of the fluid will try to get into the alveoli and what happens if you start building up a ton of water inside the alveoli? What effect does that have on surfactant production or actually surfactant concentration? It causes an increase in alveolar edema which will technically drown out the surfactant. What does surfactant do for the alveoli? Decreases surface tension. So if I smother the surfactant, what will happen to the surface tension? It will start to disappear.
As surface tension increases, what will that lead us to remember Laplace's law that says pressure is equal to twice the tension divided by the radius? As we increase the surface tension, we increase the collapse pressure, what is going to happen to this alveolar? I'm starting to collapse and now I'm going to cause an alveolar collapse and look, that's a problem because now I have tons of fluid building up around this alveolus, which affects the alveolar membrane, the respiratory membrane that allows gas exchange, that's a problem. This will lead to decreased gas exchange, that decreased gas exchange will lead to hypoxemia and that hypoxemia is a very dangerous thing, especially when it becomes refractory, so we have to be careful with that as again it releases a lot of inflammatory mediators. which cause vasodilation increased capillary permeability which leads to a lot of interstitial edema alveolar edema which smothers the surfactant increases surface tension and leads to alveolar collapse that alveolar collapse will increase the work of breathing that is another thing, it will increase the work of breathing well, then it will cause hypoxemia and will increase the work of breathing, why will the work of breathing increase?
Because now I have to work harder to try to inhale as much air as possible to not only reopen the alveolus, but also to open up against all this interstitial edema which is significantly difficult and that's what can lead them to go down the hill and drive which is called ard, well that's one thing and the next thing, all these inflammatory mediators also bring in tons of neutrophils, so now I'm going to attract neutrophils, so these inflammatory mediators will start to attract neutrophils, these neutrophils will start to come to the area and with all this inflammation they will want to start trying to destroy the virus when they start trying to destroy the virus, how will they do it?
They release reactive oxygen species. They release proteases every time I release these reactive oxygen species and proteases. Yes, maybe I can destroy some of the virus, but guess what else I'm going to end up doing? I'm going to finish. I'm damaging all these cells and as I start damaging all these different type 1, type 2 alveolar cells, what am I doing as a result of that? What do alveolar type 1 cells do? They play a role in gas exchange if I destroy them. Will I have adequate gas exchange? No, if I destroy the type 2 alveolar cells, what will that do?
My surfactant production will decrease. What will that do? It will increase the surface tension and cause the alveoli to collapse, on top of that, like everything. of these cells begin to be destroyed, begin to break off in the actual center of this alveolus, so now, in the center of the alveolus, what am I going to have? I'm going to have this whole collection here of fluid and also maybe some Protein Reservoir and Cellular Debris Type 1 Pneumocyte Cellular Debris Type 2 Pneumocyte Cellular Debris I'm going to have some macrophages here. I'm going to have some neutrophils in this area and now it just led to a consolidation.
Okay, this consolidation is going to be. a problem, okay, because this consolidation is also going to alter gas exchange and if I alter the gas exchange process, I cause hypoxemia, okay, another thing is going back, all of this can also happen when there are reactive oxygen species , it damages the type 1, type 2. alveolar cells properly and as you do that that leads to this significant alveolar collapse, we also talked about that right now, the next thing you also need to understand is that you are releasing tons of interleukin-1 and interleukin-6 inside the alveolar cells. lung parenchyma, this interleukin-1 and interleukin-6 guess where it can travel if it is released in large quantities it can travel through the blood to the central nervous system and you know that in the central nervous system there is the hypothalamus and the hypothalamus controls your temperature So interleukin-1 and interleukin-6 are in high concentrations, they tell Antoine the aquatic factor alpha, they tell the hypothalamus to release specific prostaglandins like pge2 and that helps reset this thermostat correctly and increase body temperature and that increase in body temperature goes. lead to fever, and that is important because this is one of the most common symptoms in these patients, so they present with fever, guess what else if someone has consolidations and all this type of accumulation of things inside the alveolus with the time? this starts to break down, guess what's going to happen, you're going to cough it up and when you cough, you're going to cough up this productive mucus and this could be a productive cough, so you might get a productive cough. they present with fever, they may present with increased work of breathing which may present as dyspnea or difficulty breathing and perhaps they could even have some hypoxemia as well due to someone's hypoxemia.
What happens as a result of that? What triggers that? If they really remember. quickly, if someone has a low partial pressure of oxygen that stimulates what are called chemoreceptors correctly, then it stimulates their chemoreceptors. When the po2 is really low, it can stimulate the actual peripheral chemoreceptors and those chemoreceptors can do what they can actually trigger a reflex where it actually makes the systemThe sympathetic nervous system is stimulated and tries to increase the patient's heart rate, so what else might be something to see in this patient? You may also have an increased heart rate. Well, then I could have tachycardia.
You may have more work breathing, what else does the sympathetic nervous system do too? If you are low on po2, what do you have to do to try to get more po2? increase your respirations so they may have a higher respiratory rate, they may have a higher heart rate, they may have a fever, they may have a cough, they may have an increase in the work of breathing which may present as disney or shortness of breath and maybe even hypoxemia, Let's go even a step further, let's say this starts to become as severe as this inflammation of the lung becomes so severe and it actually starts to leak into the bloodstream and spreads in this systemic inflammatory response starts to spread to different parts of the body, so now this inflammation of the lungs leads to systemic inflammatory response syndrome, or it starts as ard, so it affects the lungs, which leads to ard, maybe that progresses. to systemic inflammatory response syndrome that can lead to potentially septic shock.
How does it happen if this actual inflammation spreads throughout the circulatory system? What will he do? This will begin to cause increased capillary permeability within the systemic circulation as fluid begins to leak and accumulate within the tissue. spaces, what's going to happen to the overall blood volume, it's going to decrease, on top of that, we're going to cause vasodilation of the actual vessels as you vasodilate a lot of your systemic arteries, what's going to happen to the actual total peripheral resistance, es is going to go down as your total peripheral resistance goes down and your blood volume goes down, what is that going to do to your blood pressure?
It's going to build up and the patient can start to become hypotensive and if they become hypotensive that decreases the profusion at multiple different levels. organs and this can lead to multisystem organ failure, so this can start with just pneumonia which can then progress to the alveolar collapse that we talked about and difficulty inhaling air, which causes severe hypoxia which can become refractory and then progressing from a systemic inflammatory response syndrome to potentially septic shock, the patient becomes hypotensive afterwards, when he becomes hypotensive, he cannot perfuse his organs, how can that occur if he cannot perfuse his kidneys, what is going to happen with that bu in creatinine?
The suction is going to increase properly, so perhaps the ability to remove creatinine from the kidneys and the ability to remove blood urea nitrogen decreases because the kidneys do not receive enough blood flow, so they may have elevated levels of bu in and elevated creatinine to show that there is actually kidney damage, maybe the liver is also revved up, it's not getting enough blood flow and because of that it starts releasing specific inflammatory enzymes like ast, maybe that starts to increase, maybe the liver is altered. The enzyme starts to increase, maybe the billy starts to increase or maybe it starts to release acute phase reactive proteins.
What are some of these PCR fibrinogen, right interleukin 6? They may all be elevated, you may have elevated fibrinogen, elevated interleukin-6, and elevated CRP. liver enzymes and in fact these are some of the things that they check for in a patient that maybe comes in with this actual covid19 infection, we'll talk about that in a moment as we talk about all the different effects that can come from this. virus, which is a pretty nasty virus again from the time of infection, is fine until the patient develops symptoms, that's called the incubation period. What is the incubation period for this virus?
Currently the incubation period is the period from which it becomes infective. It is believed that between patient and patient they develop symptoms between 4 and 14 days, so that is our incubation period; however, some have seen it up to 24 days, but note that we potentially say that is a maximum of 14 days. the things that we have to keep in mind when we talk about the new coronavirus okay, let's go ahead and now move on to the diagnosis, okay, so far we talked about
epidemiology
, we talked about pathogenesis, we talked about the signs and symptoms that patients will present with right and Out of those, which were the big ones that you want to remember again, the patient comes in, has a fever, has a cough, has difficulty breathing, and sometimes you have to remember these are the most important ones: fever and then cough and difficulty breathing, but sometimes the patient can have urine symptoms or gastrointestinal symptoms, so maybe you can have rhinorrhea, congestion, sore throat, maybe a little bit of a headache, gastrointestinal symptoms can come with nausea, vomiting, diarrhea again, it's mainly fever, cough, difficulty breathing, but you can't forget that some patients may have early gastrointestinal symptoms or urinary symptoms, that's fine, but either way they have these symptoms, maybe they have had them too. tachycardic maybe they're on kipnic maybe their spo2 is a little bit lower again maybe it's less than 93 or something and you started to worry okay?What is the first step you should do? The first thing you need to remember is that sometimes this sounds. just like the flu and it could potentially be the flu, so the first thing you're going to want to do is take a sample from the patient and also ask them if they've been in contact with anyone who's been infected with the coronavirus, have they traveled outside of the United States , where there are also large numbers of infections? Those are questions you'll want to try to ask to persuade the patient to discover her actual medical history. Now, from there, take a flu test. nasopharyngeal swab and influenza test or influenza a b correct influence a influence of b so the first thing you have to do is rule out influenza, so rule out influenza a and b and how do you do that do this nasopharyngeal swab, stick this A swab is placed into the nasal cavity and tested for actual mucus to see if there are any influenza particles, so a nasal pharyngeal swab or oral pharyngeal swab can be done.
There is another thing that can also be done, well, let's say. Just because that comes out negative is not the flu does not mean that it is not yet the flu but again your suspicion is high for the corona virus because they have a very high fever, what is a fever? That's also important if a patient comes in and they have it. They have a fever and their temperature is 98.6, that is not a fever. Well, technically we consider a fever to be greater than or equal to 100.4 degrees Fahrenheit, right, that's what we consider a fever if they're coughing, if they're very short of breath.
Well, its o2. the sap maybe a little low, okay, they have tachycardia for kipnic again, you have a high suspicion. The next thing you can do is do what is called an rt pcr. Now realize that these tests have a sensitivity of what we have seen here anywhere. 30 to 80 percent and they take a lot of time, so do this test right away, but you may not get the results in time, when you need them, and also its sensitivity is not that good technically. it's the gold standard of diagnosis and you can get rt pcr from a nasopharyngeal swab or just remember you can also get it from sputum so from a sputum sample you can also get it from an aspirate that's fine and you can also get it from blood , but again you can also do a nasopharyngeal swab, okay, do an rt-pcr, which is a real-time polymerase chain reaction, that's how you can do it, it's called a nucleic acid amplification test, okay, this is very similar to what is called again, they abbreviated it as nat.
It's expensive from what I remember in my rotations they said it could cost up to $300 for the test. Well, the patient comes in and has these symptoms and again, don't forget, maybe they also have specific vital signs, meaning increased heart rate. low breathing spo2 and then worst case scenario maybe they have low blood pressure, okay that's scary but from there what are you going to do next? You'll want to do a blood test, see where the patient is, so what are they? we're going to do, we're going to order a complete blood count and a cmp and we can also, if we want, check for specific markers that have been associated with high mortality rates with this disease, so the first thing we're going to do is we're going to check a cbc cbc we it will say our white blood cell count, a red blood cell count and our platelets correctly and then we can get a difference of what we're going to see here with this and this is what's super interesting.
You see? It's called lymphopenia, eighty percent or more of the time you see lymphopenia, okay, that's really strange because what would you expect if someone has an infection? You would expect a high white blood cell count, but again, you'll more commonly see, for some reason, lymphopenia. so that's something to keep in mind, you're going to have a low lymphocyte count. The next thing you can do is ask for a cmp. A cmp can tell you a lot of different things, so with cmp it can basically be a bmp and a lfts. so let's check our IFTs, if we check the IFTs, guess what we see in patients who have this multisystem organ failure or who are a new severe case that they may have if they have decreased perfusion in the liver, increased alt. ast and billy increase, okay, that's something we can get from the lfts or the cmp.
Technically, we can also get a bmp and bmp can tell us kidney function, it can tell us electrolytes and they can also tell us our glucose level. the bmp needs to tell us what is really important if we are not receiving adequate perfusion in the kidneys, are we going to excrete as much of the bun as possible?, the nitrogen in the bloody urine, the creatinine in the urine, no, because we don't we are perfusing adequately. the kidneys are being damaged, so they may have high bu in and they may have high creatinine, which is important. The following is a test that can be done now.
Patients who get, for example, influenza, yes, they get viral pneumonia, they have a higher level. The risk of getting a super infection with a bacteria, although it leads to a specific marker that can be seen in patients with pneumonia called procalcitonin, so sometimes there is a molecule called procalcitonin, but remember that this is particular to bacterial infections, procalcitonin will be normal. you will have a normal procalcitonin level which is important if it is primarily covid19, if it is covid19 with a super infection of a bacteria then you may have an elevated pct or procalcitonin so again the only time that there will be an elevated pct or procalcitonin is if maybe there is a covid19 plus a bacterial infection, okay, and that's important to remember, the last thing you can do is check for these general markers of inflammation.
Well, what are some of these markers of inflammation? They are not specific, but they help us. in this, determining the mortality rate of the patient, one is crp, they will have an elevated crp, another is they will have an elevated esr, these are non-specific markers of inflammation, but they will be elevated, another is you. We're going to see elevated levels of interleukin 6. Where did that come from? Remember macrophages release tons of interleukin 1 6 and tnf alpha, that is one and it is also released from the liver as an acute phase reactive protein, another is when there is severe inflammation, an enzyme called lactate dehydrogenase is also found in higher concentrations .
Other things are that whenever there is massive inflammation there can also be elevated D-dimer and there can also be elevated ferritin. Well, these are all markers of inflammation that can be found in a patient with cova 19 and again these high markers can be associated with higher mortality rates, which is also very important, remember that if someone has multisystem organ failure, we can see an increase in bun, increase creatinine and we can see an increase in ast, alt and billy, what happens if there is not enough perfusion in the heart? Which we might also see elevated, so also take into account the high mortality associated with elevated troponins, troponin t ion troponin and elevated ckmb and again, this is an indicator of higher mortality rates, which could be indicative of not you're getting enough perfusion into the heart, which can also lead to a possible myocardial infarction and that can make things worse because you become hemodynamically stable and also unstable hemodynamically unstable, okay, we do all the labs to get all this information back, we're waiting for you. come back rtpcr we didn't get a positive flu now what we're going to do is take some images, usually you want to start with a chest x-ray, but you'll see that the CT scan is actually the most sensitive test right now.to be able to determine if someone has coveted 19.
Now it's not specific, which means there could be other infections, they could have influenza. or viral pneumonia such as influenza pneumonia or other different types such as adenovirus, can present real findings on a CT scan very similar to those of covid19, but again it is useful to help have a high sensitivity of 95 percent to observe the coveted 19. So the first thing you can do is get a chest x-ray. It won't be the best, but it can get you somewhere. What are some of the things you will see on a chest x-ray? this area of what's called ground glass opacities so you can see what's called ground glass opacities now from there maybe you say oh this is not that sensitive this is not what I want it's not that good I'm going to go ahead and do a CT scan, I do a CT scan and I see ground glass opacities again in the peripheral lung fields, so let's say I see some ground glass and then I go and check my actual CT scan a little bit more and then I start noticing some areas of Consolidation and if I start to see these areas of consolidation, oh, that's not good, that means I have some pneumonia as well, so we have some ground glass opacities that will be a little bit, a little bit of consolidation of interstitial edema , which will be a lot. of those actual accumulations of cell waste proteins and then they lead to what's called a special term called crazy pavement pattern so we can see the consolidation of ground glass opacities and you'll see that later when we show you on a CT scan, too you can see what's called a crazy pavement pattern, it's a special radiological term that they say can also be associated with interstitial fluid thickening and membrane thickening, as well as alveolar and interstitial edema.
Well, other things you could do is, if you have the skill or the time, you can do what's called point-of-care ultrasounds. Ultrasounds can also be used. What you can look for is what's called pleural line thickening and we'll show you what that means on an actual ultrasound so you can look for what's called pleural line thickening. Another thing you can do is you. We can check again with interstitial pulmonary edema, you can see these specific lines called b lines, so we can also look for increasing b lines within a specific area. Well, the last thing we might also see is consolidation with air bronchograms, so there may also be consolidation with air bronchograms and again we'll see all of this in the images here in just a second, okay ninja, so in this video we talk about the new corona virus or the coronavirus discovered in 2019, which is responsible for covid19 which We talk here in this video, we talk about the
epidemiology
, which included a small point on zoanosis, we talk about case fatality rates, we talk about the reproductive ratio, we talk Over the course of the series, we also go into the entire pathogenesis, how that pathogenesis produced the specific symptoms that we see in covid19, as well as practically its diagnostic process that you will look to go through and help diagnose covid19 in the following video, which What we'll do is start talking about the treatment of covid19 we'll talk about the different types of ventilation management, okay, mechanical ventilation, we'll also talk about whether the patient needs harmful antibiotics, if there's a super infection, we'll go over different prognoses, things that affect the actual prognosis, things like whether someone has underlying heart disease, lung disease, etc. and lastly, we will talk about preventive measures and how to try to reduce the spread of this very serious virus in general, Nigerians.I hope this video makes sense, I hope you guys enjoyed it, if you did please hit the like button, comment in the comment section and subscribe if you get a chance in the description box. We will have links to our Facebook, Instagram and our Patreon account. Very good engineers, as always. stay safe and see you next time
If you have any copyright issue, please Contact




![Music for Studying and Work [Easy Listening Background Music] Relaxing \u0026 Concentration](https://i.ytimg.com/vi_webp/XmuFiAamS2Y/mqdefault.webp)